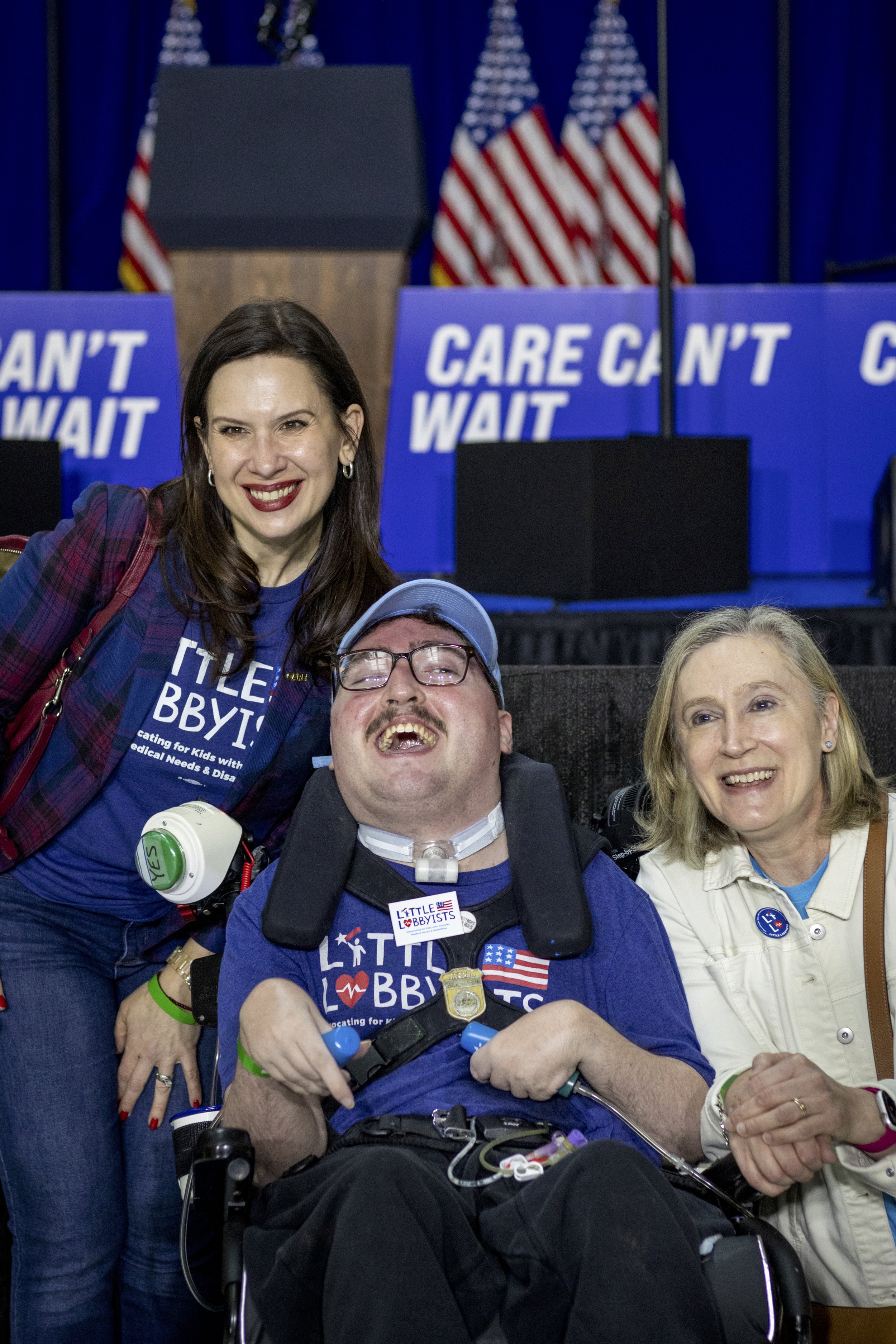
Photo Credit: Rah Studios. Image: Just some of our nationwide Little Lobbyists family at the Care Coalition’s Community Integration Summit in Washington DC! Image description: A couple dozen children of various ages and their parents pose in front of a tan and black paneled wall at the Martin Luther King, Jr. Library in downtown Washington, DC. Most of the group members wear t-shirts with the Little Lobbyists logo.
Medicaid is a life-saver for our disabled children and all disabled people. At Little Lobbyists, we’ve worked to ensure that all 50 states have a version of Medicaid’s “Katie Beckett” waiver. Even so, not all of our families can access care–waiting lists are long. Now Medicaid is at risk for everyone. Did you know that 1 in 5 persons in the U.S. are enrolled in Medicaid? That’s children, pregnant women, seniors, disabled people–and even hospital and public school systems depend on Medicaid.
Rational voices would say we need to expand Medicaid because Medicaid controls costs more effectively than other health care payers. But we are not living in rational times–we’re being tumbled as if in a huge dryer, with little sense of what to do, or which end is up.
I felt like this when my disabled son was very ill and I was expecting our second child. My therapist gave me great advice: In times of crisis, don’t think or plan more than six months ahead. Focus on what you have control over now.
I’ve stuck to that ever since. Looking too far ahead can make you panic; staying in the moment isn’t always enough. In these early days of 2025, we might modify that advice and say, “Don’t think more than one month ahead.” So what can you do this month?
Educate Others (and Yourself) About Medicaid Services
Because Medicaid is a state-federal matching program, it’s really confusing for everyday people, legislators, governors, and even Robert F. Kennedy, Jr., the nominee for U.S. Secretary of Health and Human Services. We need to educate others and ourselves.
Medicaid allows states to innovate: as a result, there are different programs for different populations in different states with different names. Many people who are on Medicaid don’t even know that it is Medicaid–and, mistakenly believing it’s a state program, don’t understand the consequences of proposed massive cuts.
You can share the following with your community, friends, and on social media:
The Little Lobbyists logo in blue, red, white and teal reads: “Little Lobbyists: Advocating for Kids with Complex Medical Needs & Disabilities.” The logo also contains an American flag, a child reaching for a shooting star, and a heart with an EKG line through it.
Caring Across Generations: 10 Things to Know About Medicaid. You can download it, too, and print it out!
Look up your state’s unique name for Medicaid services. You can click on each link to reach your state’s Medicaid services website where the names of all state Medicaid programs can be found.
Download State Medicaid Fact Sheets from the Kaiser Family Foundation (KFF) website. KFF is a highly respected nonpartisan source for health data and information. Scroll down to find more resources about different components of Medicaid. Print them and distribute them at any gathering!
Understand what changing Medicaid to block grants (aka “Medicaid per capita”) would do to limit or gut services.
Contact Your Congressional and State Legislative Representatives
It’s intimidating to call these offices. But they exist to hear from you. Legislative offices keep tallies of calls “for/against” certain bills and legislative actions, as well as cabinet appointees.
If you can only contact one office, make it your U.S. House representative. The House is narrowly divided: even a handful of votes could make a difference. Plenty of members won their seats in 2024 by slim margins. If cuts to Medicaid can’t pass the House, any Senate bill is compromised as well. Likewise, the nomination of RFK Jr. has run into obstacles and you can tell your rep to vote no.
Call or write both your congressional and state representatives. Calling is best. While the U.S. Congress can vote to slash federal funding, state governments also make Medicaid decisions and state dollars go toward those services.
If you call, here’s a quick script. Remember to be polite to the person answering the phone. You can keep it brief, or go into more detail as you like.
“I am your constituent [your name] from [city/town] and my zipcode is [x]. My [family member/friend] depends on Medicaid to live at home where he/she/they belong and stay out of an institution. Please do not cut Medicaid funds. [Quote a Medicaid fact about your state.] You are only hurting your own constituents.”
If you want specifics about your representative’s stance, ask to speak with the Legislative Assistant (LA) who handles health care. You may end up leaving a voice message, but that’s ok.
Calling is the most effective way to make your position known, but you can also send a message through the website of your U.S. senator or representative. Look for a button on the “Contact Me” page through which constituents can share their opinion.
Take a Deep Breath
Despite the fact that we are constantly being advise to “take care of yourself,” and our response is often, “how?,” do find five or ten minutes to do a crossword puzzle, chat with a friend, take a walk, or listen to your favorite songs.
And, stay tuned. We’re in this together. Share this post with your friends!
Jeneva Stone and her son Rob are members of Little Lobbyists. Jeneva is the Little Lobbyists blog manager.
























































































![Sierra as a child during a hospitalization. [image description: A young white girl with short black curly hair stands holding onto an IV pole mounted with various medical devices. She wears a black pajama shirt and pink patterned pajama bottoms.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1619109871858-LH2M2CRD7WQK46LY0X2T/Sierra%2Btransplant%2B2.jpg)
![Sierra today. [image description: A young white woman with long curly blonde hair is seated outdoors. She wears a scoop-neck burgundy top and a burgundy and black checked skirt.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1619110000522-FCFU7LPA6G70W03G3NRM/Sierra+graduation.jpg)























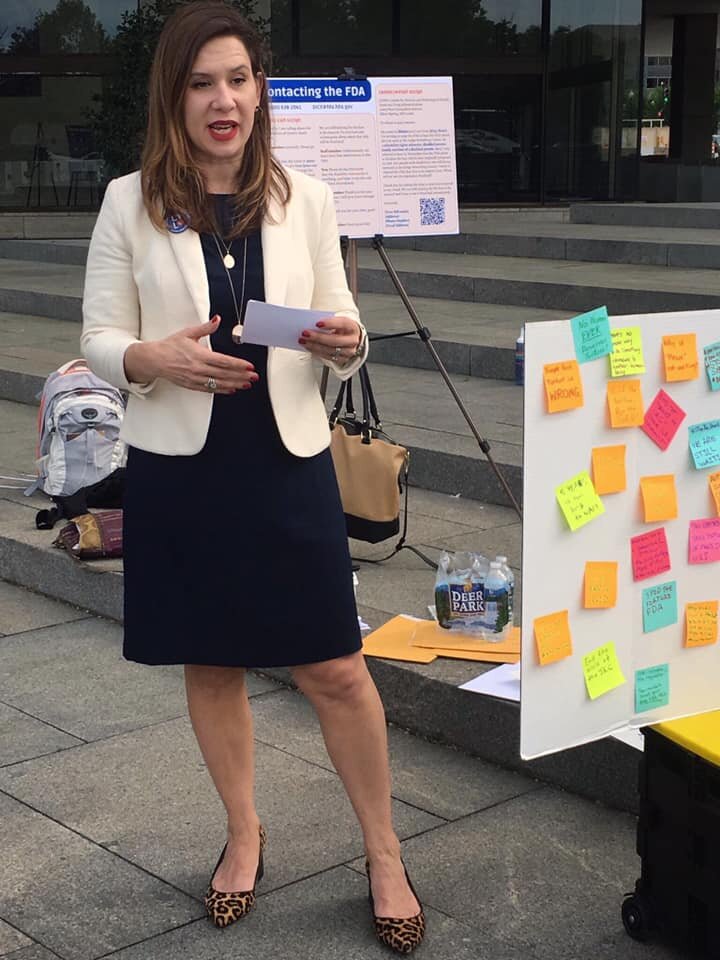
![[image description: Little Lobbyists mom and director of operations, Tasha Nelson, speaking at the podium of a press conference for affordable pharmaceuticals.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1570982613972-N1LIBT0JYAWQLAQXFZNU/Tasha+at+the+podium+of+a+press+conference+for+affordable+pharmaceuticals)